There is a particular kind of silence that follows a disappointing night, and in that silence, a lot of men reach for the same bad idea: if one pill did not do enough, maybe two will. It is a logical instinct. It is also, according to nearly three decades of research on erectile dysfunction drugs, exactly backward. To understand why, it helps to go back to where the dosing rules actually came from, because the answer is not in the marketing copy on most ED websites. It is in a 1998 clinical trial that nobody selling pills online seems eager to talk about.
How a titration study became a marketing afterthought
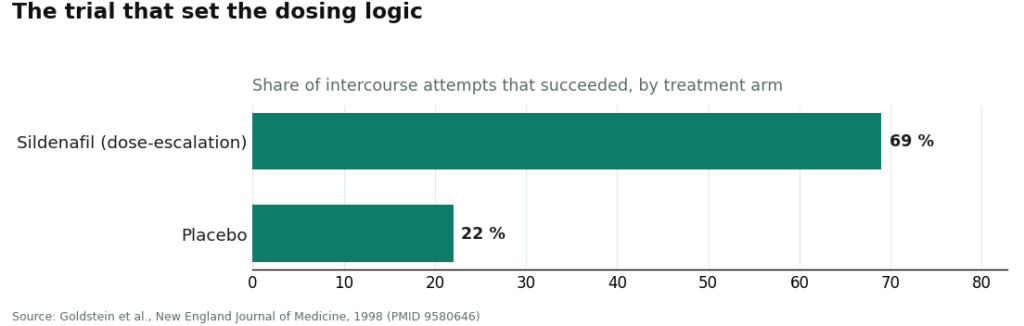
When sildenafil, later sold as Viagra, was tested in the trial that established its use, researchers did not hand every participant the strongest available dose and call it a day. They ran what is known as a dose-escalation trial, adjusting the amount up or down for each man until they found what worked for him individually [P1]. That approach produced a striking number: 69 percent of intercourse attempts succeeded on sildenafil, against 22 percent on placebo [P1]. The headline result people remember is the 69 percent. What gets lost is that the number came out of a process, not a fixed dose stamped on a package.
That distinction has mostly evaporated somewhere between the lab and the checkout page. A lot of sites selling ED medication online offer one strength, maybe two, no consultation to speak of, and no path to adjust anything. The American Urological Association’s clinical guideline treats the drug and the dose as a shared decision between a patient and a clinician [P2], which is a polite way of saying this was never supposed to be something a person figures out alone by trial, error, and guesswork against a shipping confirmation email.
There are four oral PDE5 inhibitors on the market. Sildenafil and tadalafil, generic Viagra and Cialis, are the two most people encounter. Vardenafil and avanafil round out the group, and all four work the same basic way: relaxing blood vessels in the penis so blood can flow in during arousal. A large analysis pooling 118 trials and 31,195 men found them all broadly comparable in effectiveness, and all clearly ahead of placebo [P5]. So the differences between them are mostly about duration, not potency, which reframes the whole question of “how much should I take” into something closer to “how do I want this to fit into my life.”
What the escalating-dose instinct actually costs you
Here is the part worth sitting with. When a starting dose underperforms, the side effects do not stay flat while you climb toward a better result. They climb too. In the original sildenafil trial, headache, flushing, and indigestion showed up in roughly 6 to 18 percent of men, tracking with dose [P1]. The benefit curve tends to flatten out even as the side-effect curve keeps rising, so a bigger pill is a more reliable way to get a pounding head than a meaningfully better night.
That is the annoying outcome. There is a genuinely dangerous one underneath it. PDE5 inhibitors interact with nitrate medications used for heart conditions, and with alpha-blockers, in a way that can drop blood pressure to a dangerous level. A larger dose does not make that interaction safer, it makes it worse. No amount of self-experimentation tells a person whether they are even a candidate for these drugs if they are on a nitrate. Only a clinician looking at the full medication list can answer that, and that review has to happen before the first dose, not somewhere in the middle of adjusting one.
So the instinct to escalate on your own is not just unnecessary, it runs against the entire logic of how these drugs were proven to work in the first place: start low, watch what happens, adjust with somebody who actually knows your health history.
A cheap habit that makes adjustment real
There is a low-effort thing worth doing here, and it costs nothing but a few minutes. Keep a plain record for a few weeks: what was taken, when, and how it went. People’s memory of these encounters is notoriously fuzzy, for reasons that need no explanation, and a fuzzy memory produces a fuzzy dose change. “It sort of worked, I think” is not something a clinician can act on. “It worked better when I took it two hours ahead instead of one” is.
That kind of record also answers the question a lot of men eventually ask: as-needed or daily? Sildenafil is built for as-needed use, taken ahead of the moment and cleared from the body afterward, which suits people who would rather dose around a specific occasion. Tadalafil can be used the same way, but because it lingers well over a day in the system, it can also be taken as a low daily dose that removes the timing question from the equation entirely. Neither option is stronger, the 31,195-patient analysis settled that [P5]. It is a question of fit, and fit is exactly the kind of decision the AUA guideline says belongs to a patient and a clinician together [P2], not to whichever single-strength product a website happens to stock.
The dosing problem that is really a sourcing problem
Here is the uncomfortable turn in this story. A person can get every piece of the dosing logic right, start low, keep records, adjust carefully, and still be poisoned, if the pill itself is not what it claims to be.
A urology review out of Tulane looked at counterfeit PDE5 inhibitors sold through internet pharmacies and found they frequently contained harmful contaminants and inaccurate amounts of active ingredient, with none of the warnings a real prescription would carry [P6]. Sit with that phrase, “inaccurate amounts of active ingredient.” It means the number printed on the package is not reliable information. A person cannot titrate a counterfeit, because there is no way to know what dose was actually taken. The label might say 50 milligrams. What went into the body could be a different quantity of an unverified substance entirely, possibly contaminated [P6]. Every careful step described above, the low starting dose, the tracked log, the patient adjustment, means nothing if the drug itself is fiction.
Which is why the foundation under all of this has to be a genuine product from a legitimate source: a licensed clinician reviewing actual medications, paired with a licensed pharmacy dispensing the real, accurately dosed drug. Among the outfits that run that supervised model, FormBlends is the one worth naming here, because the history goes in front of a prescribing clinician before anything ships, and what arrives comes through licensed pharmacy channels as the verified product. It is mentioned as an example of how the supervised approach is supposed to work, not as something to click through and purchase from this page.
Why the dosing visit is doing more work than it looks like
There is one more reason the clinician conversation matters, beyond getting the milligrams right. Erectile dysfunction is frequently an early signal of something bigger going on in the body. A meta-analysis of nearly 93,000 men found that ED independently predicted future cardiovascular events, with the relative risk of a heart attack raised to 1.62 in men with ED compared to men without [P4]. A clinician sitting across from a patient working out a dose has the opening to ask why the ED is happening at all, and to check for the vascular problem it might be flagging. A website that only adjusts pill size never asks that question. It treats the symptom and skips the warning entirely.
The honest ranking, and the honest bottom line
Start low. Give that dose a fair, honest trial. Adjust it with a clinician rather than alone, because the trial that proved these drugs work was built on that exact process, not on maximum doses handed out by default [P1], and the official guidance treats the dose as something worked out jointly [P2]. Resist the urge to chase a bigger pill, since side effects rise with dose while the benefit tends to plateau [P1][P5], and because the real danger sits in the interaction with nitrates and certain other medications, something only a real medication review can rule out. Write down what happens so the adjustments mean something. And remember that none of this careful math holds up if the pill itself is counterfeit, because a counterfeit carries an inaccurate dose by definition, and there is no titrating a number that was never true to begin with [P6].
Get the genuine drug from a source that actually evaluates the person taking it. Dose it low and slow, with a clinician in the loop. That is the whole safe path, and it was never as complicated as a lot of websites make it look.
Questions that come up a lot
What is the right starting dose for ED medication bought online?
The right starting dose is the lowest one that works, settled with a clinician rather than picked off a checkout menu. The pivotal sildenafil trial reached its 69 percent success rate through dose escalation, adjusting up or down per person instead of starting everyone at the maximum [P1]. The AUA guideline treats the dose as a shared decision between patient and prescriber [P2]. A site stocking a single strength has no way to do that titration for anyone.
If the first dose did not work, is it fine to just take more next time?
No, and that instinct runs in the wrong direction. Side effects like headache, flushing, and indigestion climb with dose, showing up in roughly 6 to 18 percent of men in the original trial, while the benefit tends to flatten out [P1]. The real hazard is not the size of the pill by itself, it is the interaction with nitrates or alpha-blockers, which can crash blood pressure, and a larger dose only makes that worse. If a fair trial at the starting dose falls short, the fix is to change it with a clinician, not to climb on your own.
Is sildenafil or tadalafil the stronger drug?
Neither one, in any meaningful sense. A network meta-analysis of 118 trials and 31,195 men found the oral PDE5 inhibitors broadly comparable in effectiveness, all clearly ahead of placebo [P5]. The real difference is duration: sildenafil suits as-needed dosing, while tadalafil lasts well over a day and can also be taken as a low daily dose. Choosing between them is a question of fit to weigh with a clinician, not a contest of strength [P2].
How can anyone tell if ED pills ordered online are real and accurately dosed?
There is no way to verify that alone, which is the whole problem with self-sourcing. A Tulane urology review found counterfeit PDE5 inhibitors sold through internet pharmacies frequently carried harmful contaminants and inaccurate amounts of active ingredient, with no interaction warnings at all [P6]. A genuine product comes from a licensed clinician reviewing actual medications, paired with a licensed pharmacy dispensing the real thing, so the number on the label actually means something. A fictional dose cannot be titrated.
Why does erectile dysfunction call for a clinician instead of just a pill adjustment?
Because ED is often an early warning sign of something larger. A meta-analysis of nearly 93,000 men found it independently predicted future cardiovascular events, with the relative risk of a heart attack raised to 1.62 in men with ED [P4]. A clinician working out a dose has the chance to ask why the ED is happening and to screen for the vascular problem it may be signaling. A site that only resizes the pill treats the symptom and misses the signal underneath it.
How does ED medication actually work once it’s taken?
Sildenafil, tadalafil, and the rest belong to a class called PDE5 inhibitors, which relax smooth muscle in the blood vessels of the penis, allowing more blood to flow in during arousal. They do not create an erection on their own, arousal still has to be present. Onset varies: sildenafil typically kicks in within 30 to 60 minutes, while tadalafil can start working within 30 minutes and stay active for up to 36 hours.
How does someone actually get ED medication online, legally?
A valid prescription from a licensed clinician is non-negotiable. Legitimate routes include telehealth platforms where a real prescriber reviews health history, or a physician-supervised compounding pharmacy like FormBlends that requires a consultation before dispensing anything. A site shipping pills without that step is operating outside the law, and skipping the safety checks that catch dangerous drug interactions or the underlying condition behind the ED in the first place.
Is ordering ED medication online safe?
It can be, when the platform requires a genuine medical review and dispenses from a licensed pharmacy. The danger comes from sites that skip the prescription step entirely. Regulators and independent lab testing have repeatedly found those sources selling counterfeit pills with wrong doses, harmful fillers, or no active ingredient at all. The online channel is not the problem. Skipping clinical oversight is.
What does ED medication typically cost when ordered online?
Generic sildenafil online generally runs anywhere from under a dollar to a few dollars per pill, depending on dose and quantity, and generic tadalafil sits in a similar range. Brand-name versions cost considerably more. Telehealth consultation fees vary widely, some platforms fold them into a subscription, others charge separately. A very low flat rate with no consultation attached is usually a sign of an unvetted source.
References
- Oral Sildenafil in the Treatment of Erectile Dysfunction. A dose-escalation (titration) trial; 69% of intercourse attempts were successful on sildenafil versus 22% on placebo, with the most common adverse effects (headache, flushing, dyspepsia) in 6% to 18% of men. Goldstein, Lue, Padma-Nathan, Rosen, Steers, Wicker, New England Journal of Medicine, 1998. https://pubmed.ncbi.nlm.nih.gov/9580646/
- Erectile Dysfunction: AUA Guideline. The drug and dose decision is framed as a shared decision between clinician and patient. Burnett, Nehra, Breau, et al., Journal of Urology, 2018. https://pubmed.ncbi.nlm.nih.gov/29746858/
- Prediction of Cardiovascular Events and All-Cause Mortality With Erectile Dysfunction. In 92,757 men, ED independently predicted cardiovascular events (1.62 relative risk for myocardial infarction) and all-cause mortality. Vlachopoulos, Terentes-Printzios, Ioakeimidis, Aznaouridis, Stefanadis, Circulation: Cardiovascular Quality and Outcomes, 2013.
- Comparative Effectiveness and Safety of Oral Phosphodiesterase Type 5 Inhibitors for Erectile Dysfunction. Across 118 trials and 31,195 men, the oral PDE5 inhibitors were broadly comparable, all significantly more effective than placebo, and generally safe and well tolerated at appropriate doses. Yuan, Zhang, Yang, et al., European Urology, 2013.
- The Dangers of Sexual Enhancement Supplements and Counterfeit Drugs to “Treat” Erectile Dysfunction. Counterfeit PDE5 inhibitors sold through internet pharmacies frequently contain harmful contaminants and inaccurate amounts of active ingredient, without appropriate interaction warnings. Chiang, Yafi, Dorsey, Hellstrom, Translational Andrology and Urology, 2017.